

Practical holiday: 07/12/2025 to 08/03/2025
Dear patients,
We would like to inform you that our practice will be closed for holiday reasons from July 8nd, 2025 until, August 3, 2025.
Your practice team
Your private practice for thyroid disorders in the heart of Berlin-Mitte
Have you noticed a lump feeling or a swelling in your throat? Do you feel lethargic or depressed? Are you irritable or suffering from mood swings? Do you sweat a lot? Have you noticed cardiac arrhythmia? Do you suffer from hair loss or inexplicable weight changes? All these symptoms can be signs of a disorder of the form or function of the thyroid gland.
Dr. med. Köster is a specialist in the treatment of thyroid diseases. Among other foci, this medical practice specialises in the treatment of the thyroid gland in patients who wish to have children and also pregnant women. We are a private practice; we are not registered with the statutory health insurance; therefore we only treat private patients.
Dr. med. Claudia KösterYour thyroid specialist in Berlin
 Dr. med. Claudia Köster gained her degree in medicine from Hanover Medical School (MHH/Medizinische Hochschule Hannover); there she also completed her specialist training in the Department of Nuclear Medicine and special Chemistry. In 1996 she completed her specialist training with the specialist medical state examination.
Dr. med. Claudia Köster gained her degree in medicine from Hanover Medical School (MHH/Medizinische Hochschule Hannover); there she also completed her specialist training in the Department of Nuclear Medicine and special Chemistry. In 1996 she completed her specialist training with the specialist medical state examination.
During her specialist training at Hanover Medical School, her main research interests were the quantification of myocardial perfusion by means of positron emission tomography and thyroid carcinomas with a special focus on the medullary thyroid carcinoma.
Dr. med. Claudia Köster received her PhD in 1992 upon having submitted her PhD thesis on comparative experimental work on metabolic changes in rat liver as a result of alcohol and hyperthyroidism.
Since 1997 Dr. med. Claudia Köster has been practicing as a specialist in nuclear medicine in Wolfsburg, Germany. In the course of her work she has been increasingly specializing in thyroid diagnostics and therapy.
Dr. med. Claudia Köster is married and has four children.
Thyroid diseases
There are many different thyroid diseases. The thyroid gland can be enlarged, but it may also be very small. Even in a normal-sized thyroid gland there may be lumps, which often do not cause any problems. These thyroid nodules can be differentiated into "hot" and "cold" thyroid nodules.
It is not uncommon for inflammations of the thyroid gland to occur, which often lead to functional disorders of the thyroid, i. e. hyperthyroidism and hypothyroidism, the latter also called hypothyreosis. Also, thyroid carcinoma (thyroid cancer) can occur in the thyroid gland.
Thyroid gland disordersSymptoms
Hyperthyroidism
Hyperthyroidism is a functional disorder of the thyroid gland that may occur as a result of acute or chronic inflammation. Hyperthyroidism can also be caused by thyroid autonomies or by an overdose of thyroid hormones.
The typical symptoms of an overactive thyroid gland are mental agitation, palpitations, irritability, weight loss and sweating, but it can also occur completely without symptoms.
An overactive thyroid gland leads to heart stress and always needs to be treated. Depending on the underlying disease, this can be treated with medication, surgery or radioiodine therapy.
Hypothyroidism
An underactive thyroid gland (hyothyroidism) is a functional disorder that may occur as a result of inflammation (eg. Hashimoto). It can also be the result of radiotherapy or surgery.
The hypofunction of the thyroid gland can be accompanied by symptoms such as slackness, tiredness, listlessness, depressive moods, weight gain or headaches. Some patients have no symptoms at all.
The hypofunction of the thyroid gland does not necessarily have to be treated with medication.
Goiter
The enlargement of the thyroid gland is called goiter. It occurs with or without nodules. In the case of throat problems, drug therapy may be necessary. In rare cases, surgery or radioiodine therapy may be necessary.
Autonomy
Hot nodules are nodules that produce increased amounts of thyroid hormones. They are always benign. They can lead to hyperthyroidism. An overactive thyroid glad can cause symptoms such as anxiety, palpitations, weight loss and sweating.
Cold Nodules
Cold nodules often occur in the thyroid gland. They do not produce hormones. Therefore they do not change the thyroid metabolism. In most cases cold nodules are completely harmless. Very rarely, however, they can degenerate malignantly. Thus they must be checked regularly and sometimes need to be removed.
Graves' disease
Graves' disease is an autoimmune-induced chronic inflammation of the thyroid gland, which is often accompanied by hyperfunction, i. e. an increased production of thyroid hormones.
The overactive thyroid in Graves' disease can be accompanied by symptoms such as mental agitation, palpitations, sweating and weight loss. Sometimes, Graves' disease can also cause thickening of the eyes, the so-called endocrine orbitopathy.
Autoimmune thyroiditis
Autoimmune thyroiditis (M. Hashimoto or M. Ord) is a chronic, autoimmune disease of the thyroid gland, often accompanied by the symptom of a scarring shrinkage and hypothyroidism.
It can cause symptoms such as freezing, lethargy, listlessness and weight gain. In rare cases, autoimmune thyroiditis can also lead to growth of the thyroid gland. This rampant form of thyroiditis is called Hashimoto's thyroiditis.
Thyroid carcinoma (thyroid cancer)
Thyroid carcinomas are rare. However, there are many thyroid nodules. The problem is to recognize the few degenerated nodules so that a thyroid carcinoma can be treated early.
Thyroid tumors, both the differentiated thyroid carcinomas and the medullary thyroid carcinomas, have an excellent prognosis if detected early enough. They grow very slowly. They form metastases in the body very late, so that this type of cancer is usually treated early enough. Only the undifferentiated (anaplastic) thyroid carcinoma is a fast growing tumor. It occurs very rarely nowadays, which may be due to the increasing iodination of food.
In rare cases a cancer in the thyroid gland may not have grown there but may be a metastasis of another tumor (lung cancer, breast cancer, kidney cancer). Fortunately, these metastases are rarely found.
Thyroid gland & pregnancy
During pregnancy a normal thyroid function is very important. An underfunction of the thyroid gland leads to an increased miscarriage rate during pregnancy.
As early as in the phase when there is a desire to have a child, too low thyroid hormone levels lead to a reduced ability to conceive. Pregnancy should be avoided in cases of hyperthyroidism.
Most of the medications used to treat hyperfunction are harmful to the unborn child – depending on the dosis. However, failure to treat hyperfunction is also harmful to mother and child. In the case of goiter formation, a therapy of the thyroid gland should be effected during pregnancy because pregnancy stimulates growth of the thyroid gland and thyroid nodules.
The thyroid gland and pregnancy
Hypothyroidism
During pregnancy a normal thyroid function is very important. An underfunction of the thyroid gland leads to an increased miscarriage rate during pregnancy. As early as in the phase when there is a desire to have a child, too low thyroid hormone levels lead to a reduced ability to conceive.
There are studies that link too low maternal thyroid hormone levels during pregnancy with a slightly lower intelligence quotient of the child.
Substitution therapy
If maternal hypothyroidism is known to exist, thyroid hormone therapy must be optimized before pregnancy.
The values must then be checked immediately in the pregnancy to prevent miscarriage in early pregnancy. In the further course of the pregnancy regular laboratory checks must also be carried out. If the mother's values are always well adjusted during pregnancy, there should be no negative consequences for the child.
Hyperthyroidism
Pregnancy should be avoided in cases of hyperactivity. Most medicines for hyperactivity (thyrostatics) are harmful to the unborn child, depending on the doses.
Failure to treat hyperfunction in pregnancy is also harmful to mother and child.
Goiter
In case of goiter formation, thyroid therapy should be carried out during pregnancy, because pregnancy stimulates growth of the thyroid gland and also of thyroid nodules.
The parameters of the therapy must be checked regularly.
Thyroid gland diagnosticsExamination procedure
The diagnosis of the thyroid gland consists of various examinations: Manual palpation, ultrasound examination (sonography) of the thyroid gland and the lymph nodes of the neck, and laboratory tests.
The complete examination of the thyroid gland is usually performed at the time of your appointment.
If you have already had earlier thyroid examinations, please bring the reports of your previous examinations or thyroid surgery to your examination appointment as this will make it easier for Dr. Köster to assess your thyroid.
In individual cases, a scintigraphy of the thyroid gland to assess the nodules, a trachea image (X-ray examination of the trachea) to clarify a constriction caused by the thyroid gland, or an MRI or CT of the thorax (magnetic resonance tomography or computer tomography of the thorax) are necessary to identify any parts of the thyroid gland which may be located in the thorax. We will issue a transfer certificate to the pertinent specialist for these examinations.
Dr. Köster will discuss the further procedure with you directly after the examination. Of course, you or your family doctor will also receive a detailed written report after about 14 days.
Laboratory diagnostics
The blood serves to determine the thyroid function, thyroid inflammation can be detected, and also indications of thyroid tumors can be found.
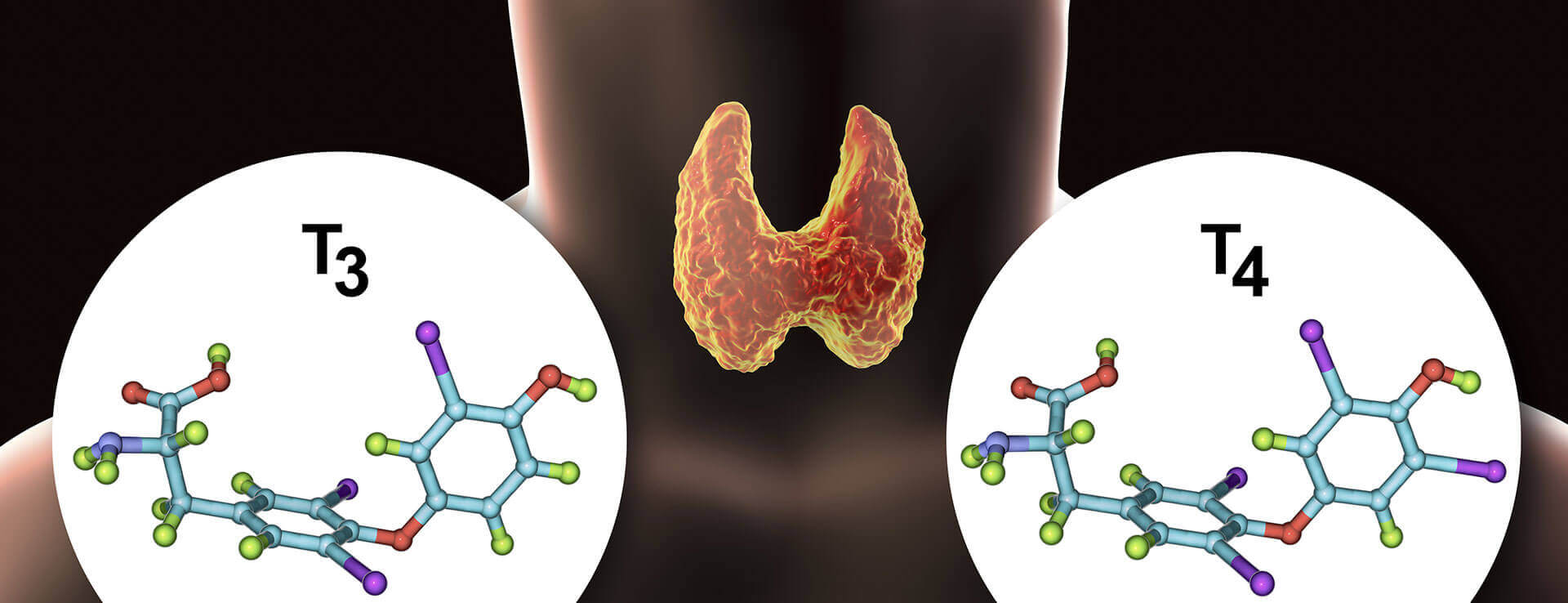
To detect or rule out hyperthyroidism or hypofunction of the thyroid gland, the thyroid hormone levels (T3 and T4) and the thyroid stimulating hormone (TSH) as the controlling hormone of the pituitary gland are determined.
All thyroid hormones are strongly protein-bound, and therefore the volumes fluctuate. However, the important parameter is not the amount of total thyroid hormones in the blood anyway, but the free portion of thyroid hormones that is functionally active. This is why nowadays free thyroid hormone levels (fT3 and fT4) are usually determined. Thyroid autoantibodies occur in autoimmune diseases of the thyroid gland, which are very common these days.
In autoimmune thyroiditis (Hashimoto's thyroiditis), often there are increased values of the TPO antibodies (antibodies compared to thyroid peroxidase) and Tg antibodies (antibodies compared to thyroglobulin).
Graves' disease is a disease in which TRAK (TSH receptor antibodies) are usually increased. These levels are determined to detect thyroid inflammation or to monitor the course of autoimmune thyroid disease.
The thyroid tumour markers are thyroglobulin and calcitonin. They indicate the presence of thyroid carcinoma.
Thyroglobulin is often increased in papillary or follicular thyroid carcinoma and is particularly important in the aftercare of these thyroid tumours. However, thyroglobulin may also be high in benign thyroid nodules (follicular neoplasia), but is usually also increased if there is an acute inflammation of the thyroid or bleeding into thyroid nodules or cysts. For this reason the values must always be compared with the other findings of the thyroid examination.
Calcitonin is a tumour marker that is very accurate in detecting medullary thyroid carcinoma. Calcitonin is also extremely important in the follow-up care of medullary thyroid carcinoma after surgery. Calcitonin can also be increased in benign thyroid diseases (C-cell hyperplasia), but also in kidney diseases or, but rarely, in bronchial carcinoma or breast cancer.

Thyroid sonographyUltrasound examination
With the help of sonography (ultrasound examination), structural changes in the thyroid gland (nodules, cysts, calcifications) can be found, the size of the thyroid gland can be determined, or tissue changes can be observed.
Our colour Doppler sonography device DC-60 Expert (Mindray) works in a frequency range from6 MHz to 14 MHz. The innovative technology of the Combo-Wave-transducers improves the contrast and leads to a more precise detail resolution.
With our colour Doppler, the perfusion (blood flow) of the thyroid gland or structures within the thyroid gland can also be assessed. This is helpful for determining the quality of thyroid tissue.
Sometimes a sonographically controlled fine needle puncture is necessary to assess tissue, i.e. tissue removal with a thin needle under ultrasound control. This allows the tissue to be clearly assessed in the case of noticable and/or conspicuous nodules. This fine needle puncture is performed on an outpatient basis and is no more painful than a blood sample.
Thyroid scintigraphy
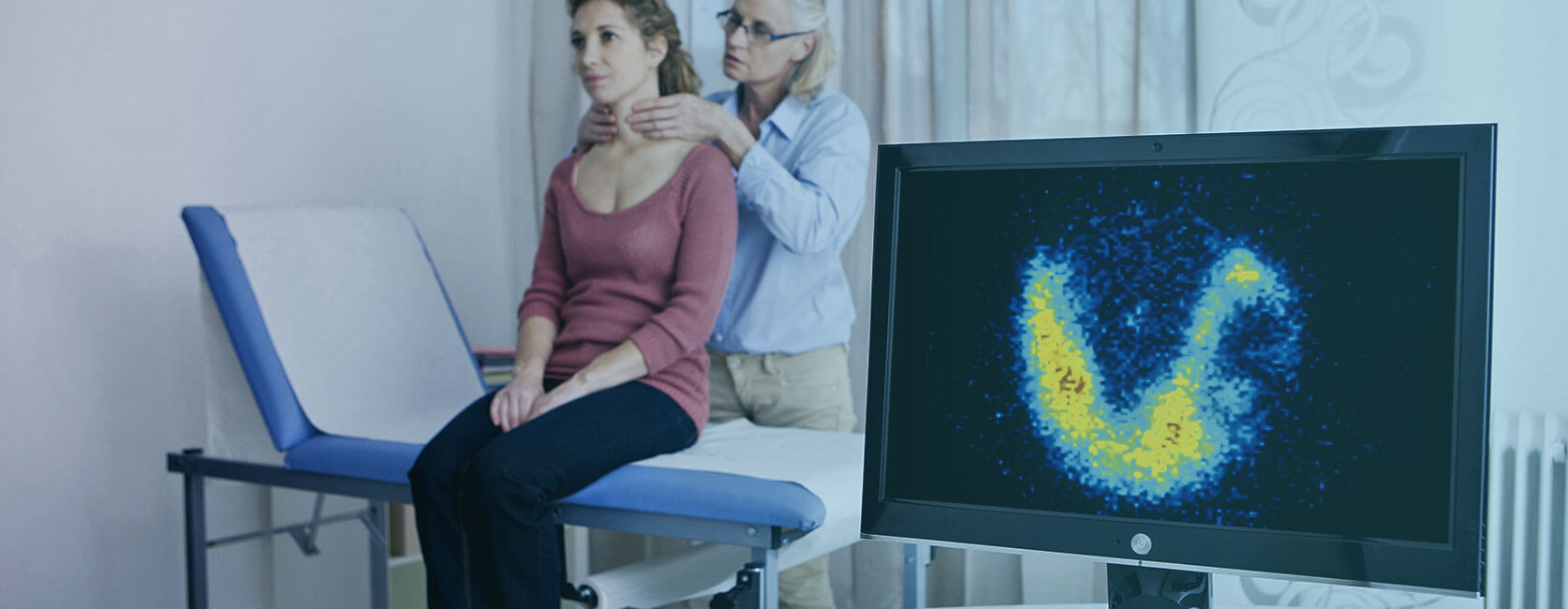
The scintigraphy of the thyroid gland is a nuclear medical examination. Often the thyroid gland can be monitored and treated well without this examination. In some cases, however, the examination is necessary.
The thyroid scintigraphy is necessary if there are noticeable nodules in the thyroid. In this case we will issue a transfer certificate to the pertinent specialist for a scintigraphy. For this examination, a slightly radioactive substance is injected into the arm vein. This substance is 99m-Technetium. The radiation exposure is very low because the technetium has a physical half-life of 6 hours and a biological half-life that is even shorter. Usually there are no allergic reactions to the injection norany other intolerances.
The technetium accumulates in the thyroid gland within 10-20 minutes. Then an image of the thyroid gland is taken with a so-called gamma camera, because the technetium emits gamma radiation. The image can then be used to show the function of the thyroid gland or individual thyroid nodules.
Hot knots can be distinguished as well as cold knots. Some nodules also have a normal metabolism. The overall metabolism of the thyroid gland can also be measured.
The hot nodules do not become malignant. They are always harmless, but they are a little less common than the cold nodules. The hot nodules can cause hyperthyroidism.
The cold nodules are harmless in the vast majority of cases. Less than 1 per mil of the cold nodules will turn into a thyroid carcinoma (thyroid cancer).
No special preparation is required for thyroid scintigraphy. The patients do not need to be fasting. They may eat and drink normally before the examination. They are also allowed to take most medications. Only thyroid tablets should not be taken on the day of the scintigraphy. The absorption of the technetium in the thyroid gland is altered if patients have been given X-ray contrast medium (e.g. in a computer tomography) in the four weeks before the scintigraphy. In such a case the examination should be postponed.
A thyroid scintigraphy is of course not carried out if you are pregnant because of the radiation exposure. With children a scintigraphy will only be necessary in very rare cases.
Appointments
If you want to make an appointment with us, please enter your name and telephone number here. We will call you back.
ContactThyroid private practice Berlin-Mitte
Location
The practice is located at Glinkastrasse 30, between Jägerstraße and Französische Straße.
Glinkastrasse 30
10117 Berlin (Mitte)
Telephone:030 / 20 05 91 33
Telefax:030 / 20 05 91 34
Appointments upon prior agreement
Mondays: 8.00 a.m.- 5.00 p.m.
Tuesdays: 8.00 a.m.- 5.00 p.m.
Wednesdays: 8.00 a.m.- 3.30 p.m.
Thursdays: 8.00 a.m.- 5.00 p.m.
Fridays: 8.00 a.m.- 1.00 p.m.
BVG (Berlin public transportation) timetable information